Lymphocyte Cells
Lymphocytes help fight disease and infection. They are primarily involved in recognizing and responding to foreign substances, such as viruses and bacteria, with two main types: T cells, which destroy infected cells, and B cells, which produce antibodies to target pathogens.
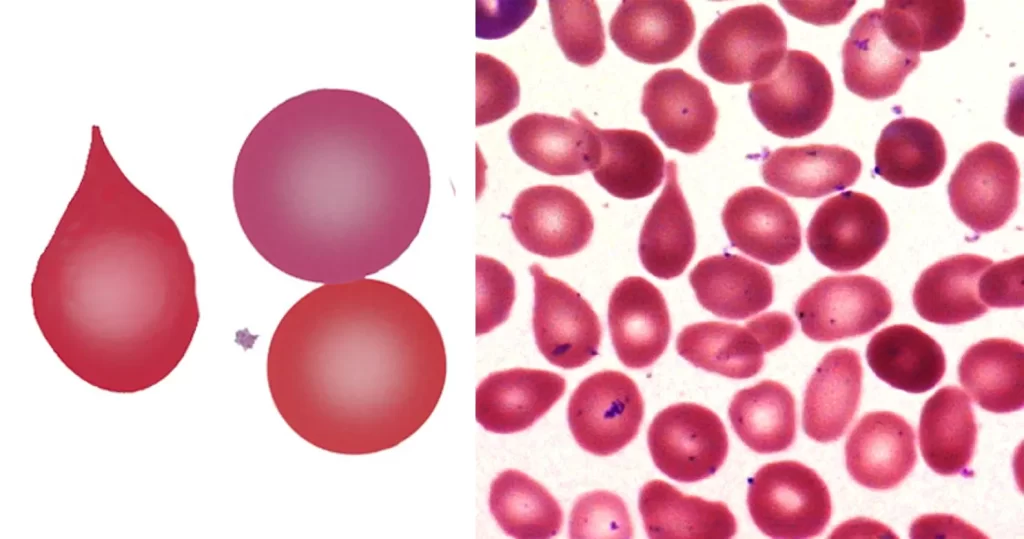
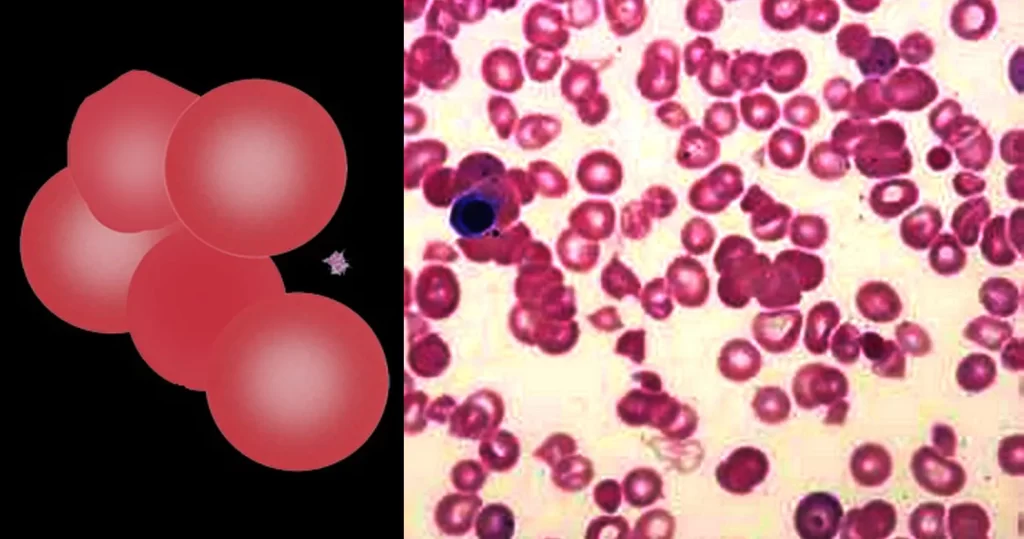
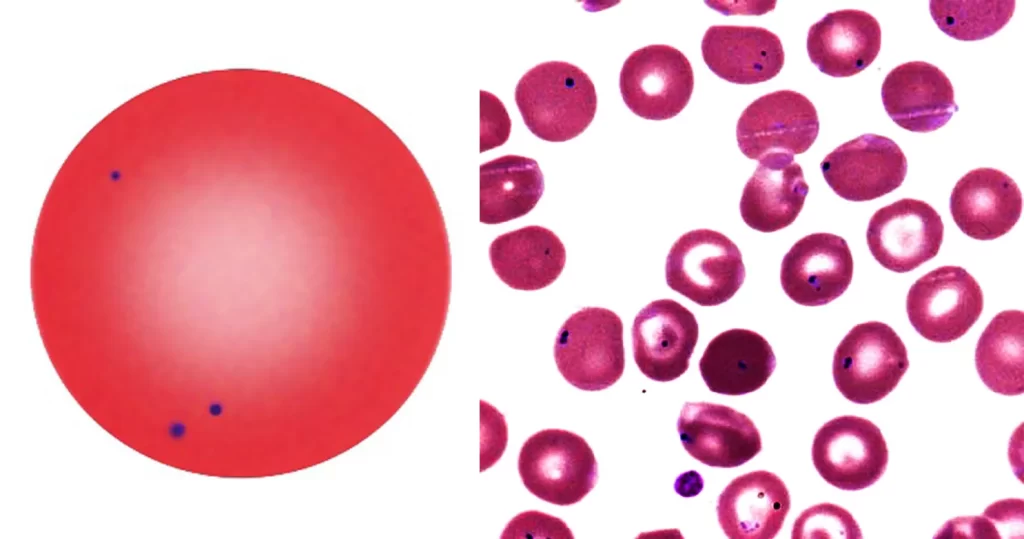
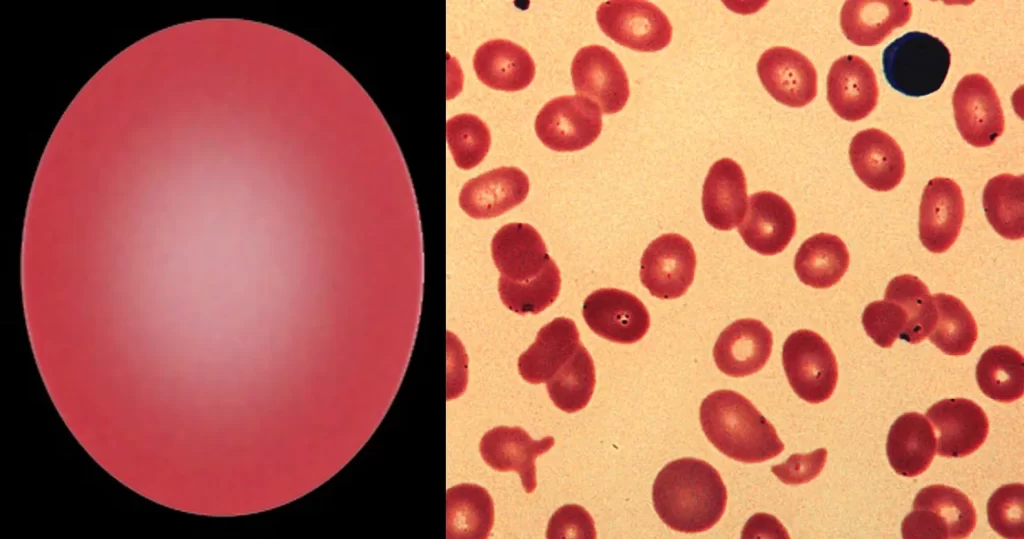
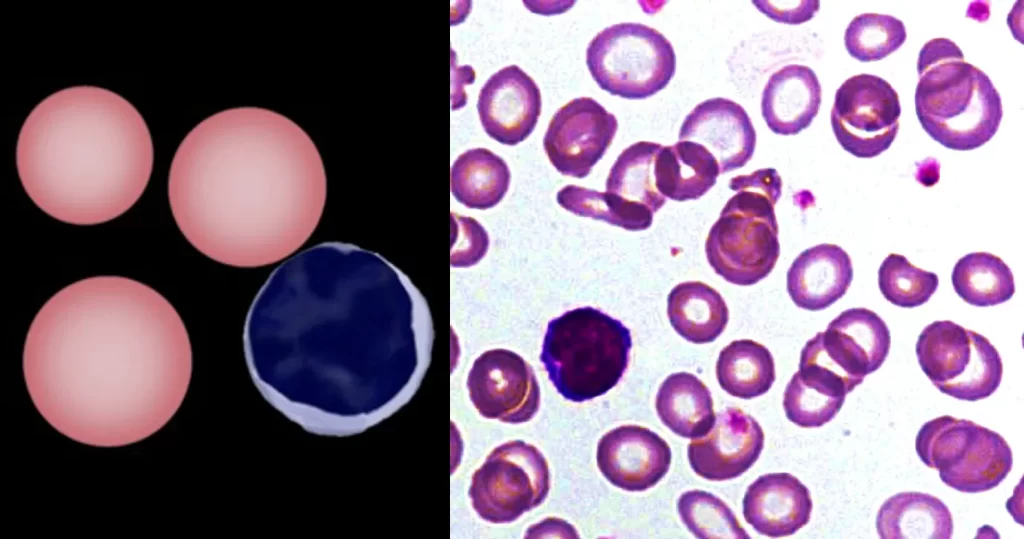
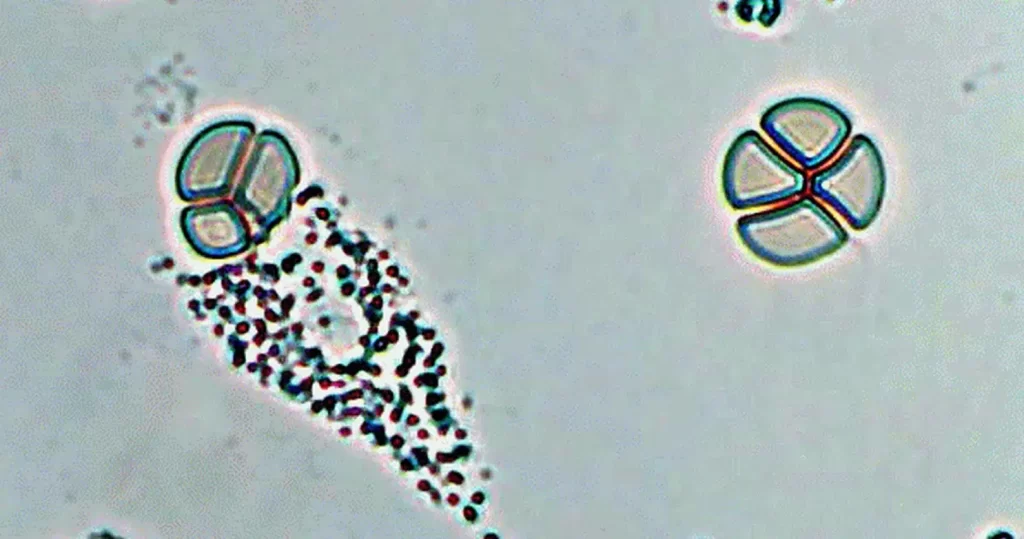
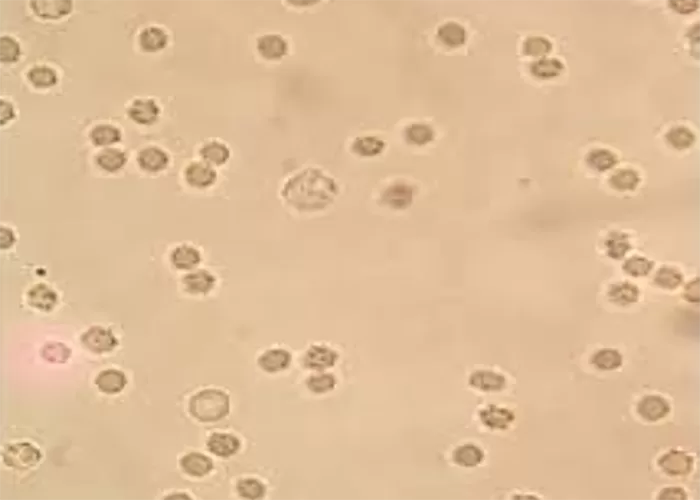
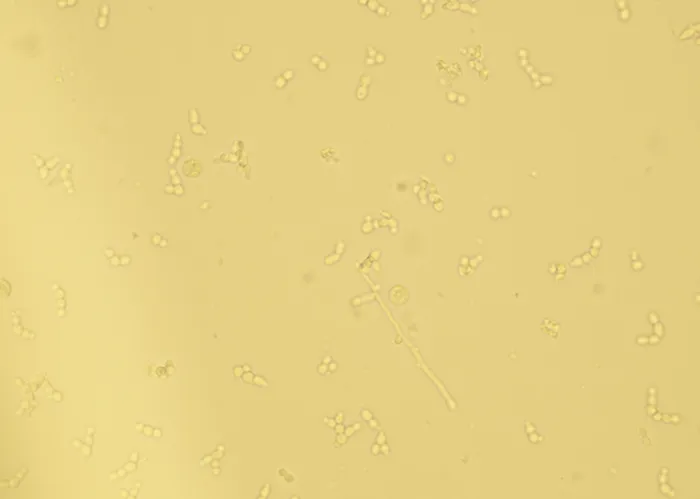
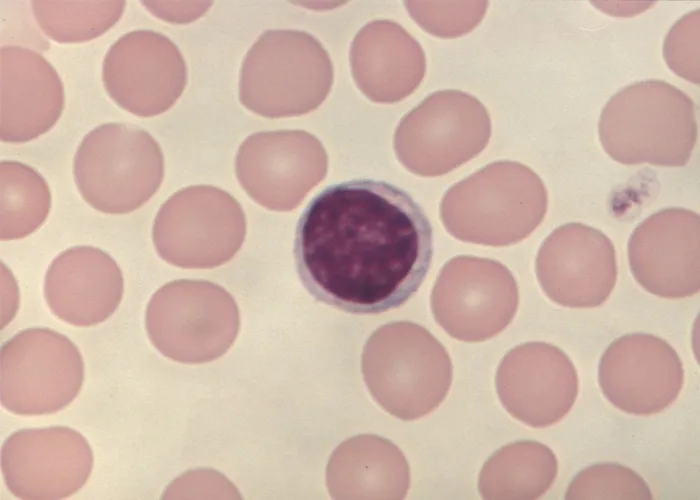
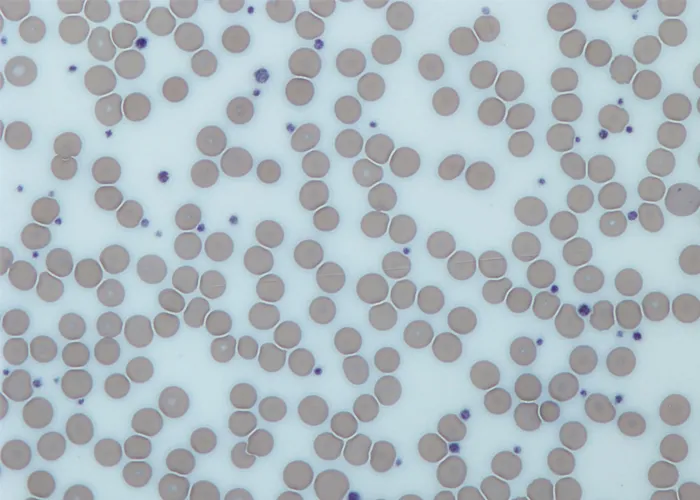
Healthy, non-active lymphocytes. An indication of no significant infection or intoxication.
http://www.medical-labs.net/lymphocytes-variation-813/
http://www.medical-labs.net/infectious-mononucleosis-and-atypical-lymphocytosis-on-asmear-188/
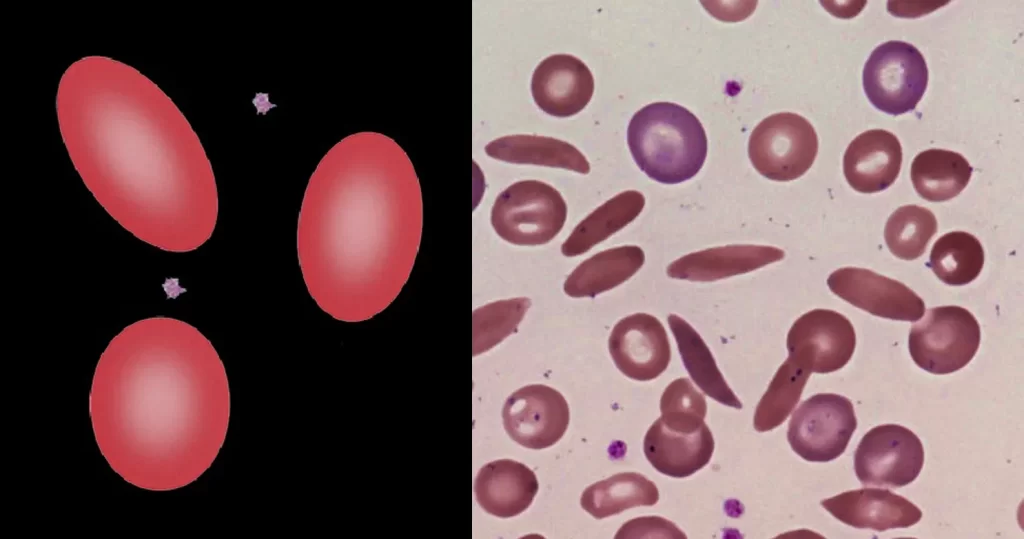
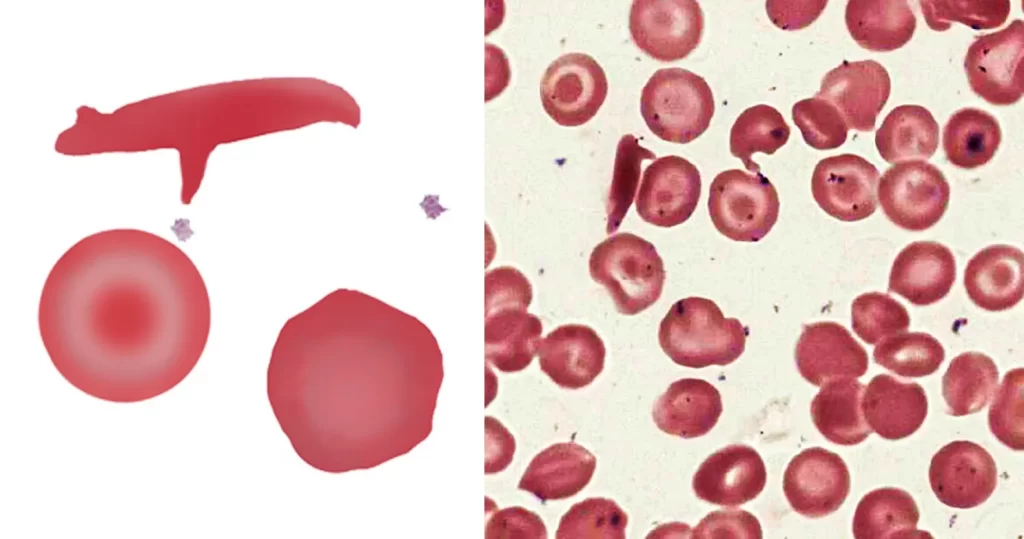
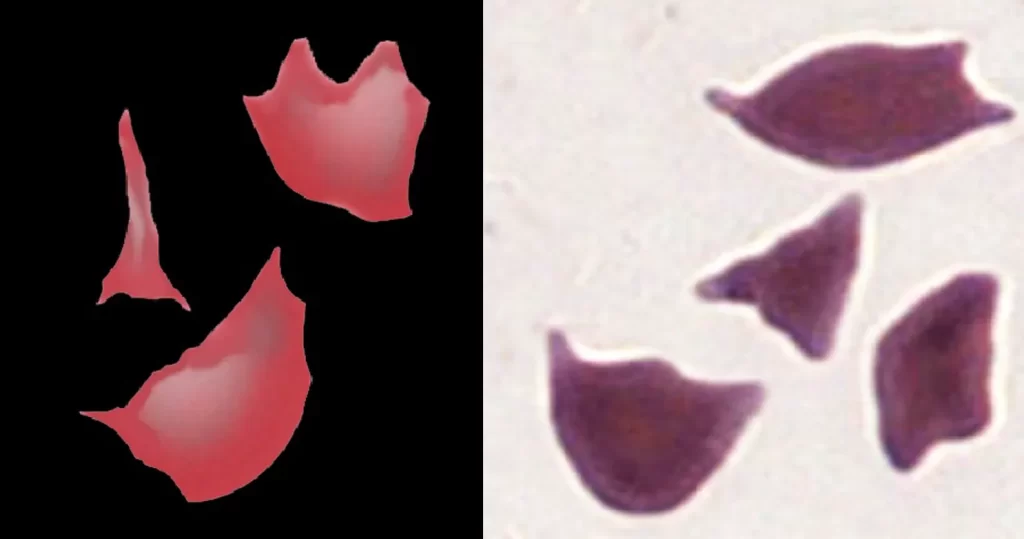
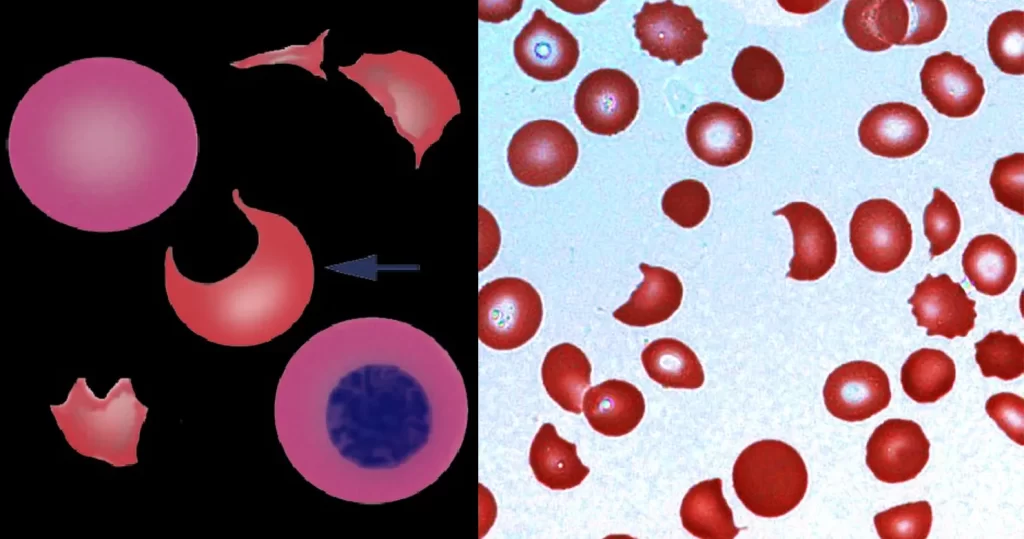
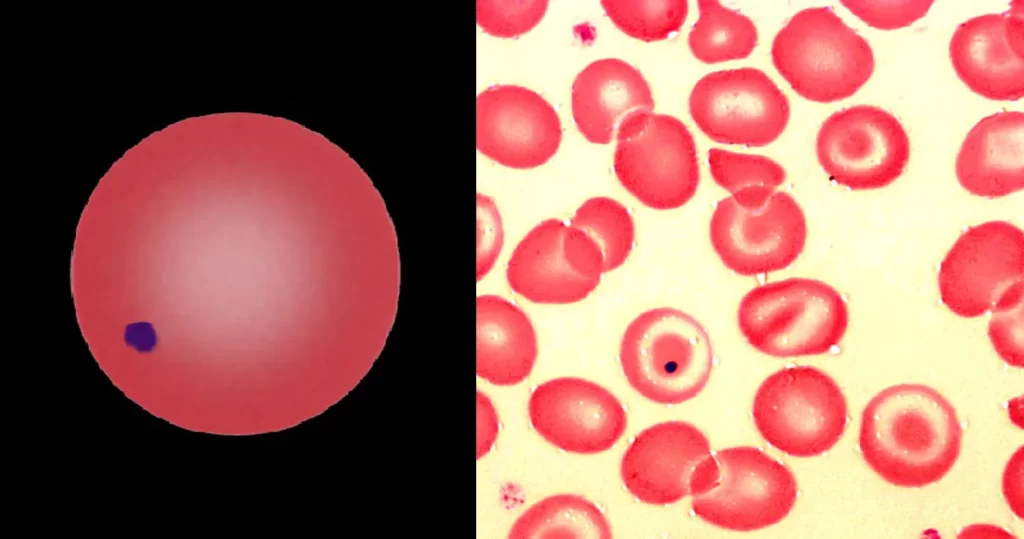
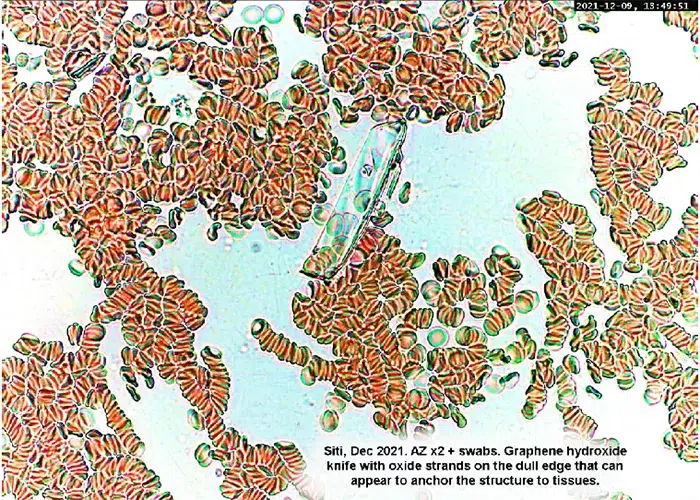
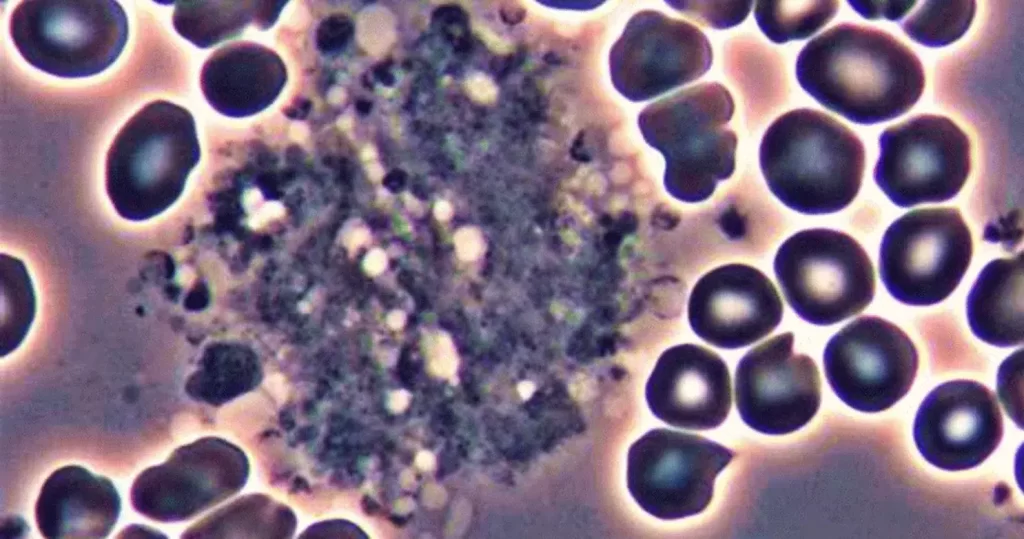
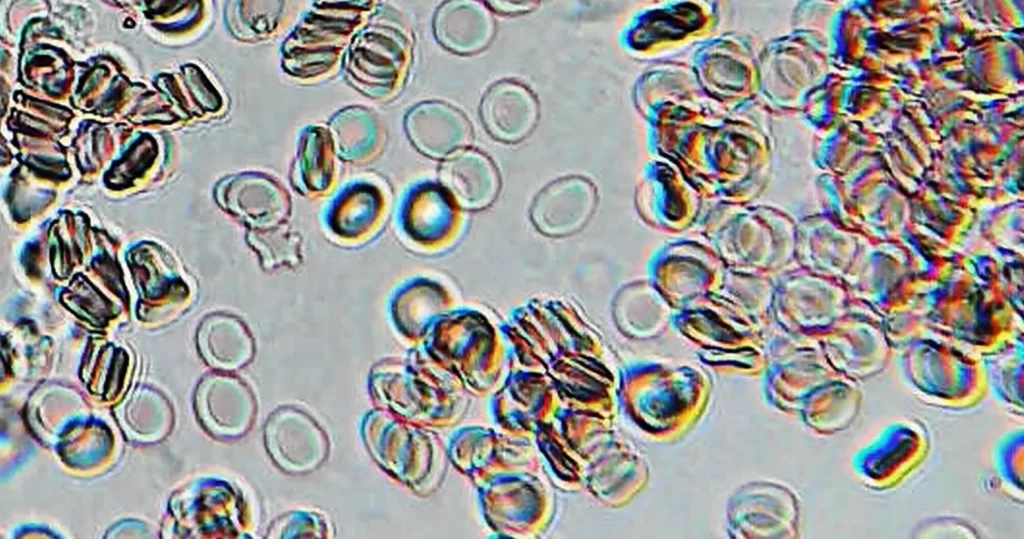
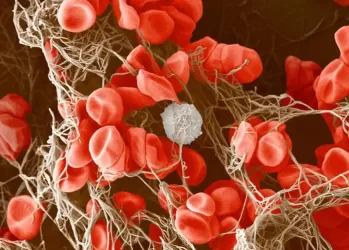
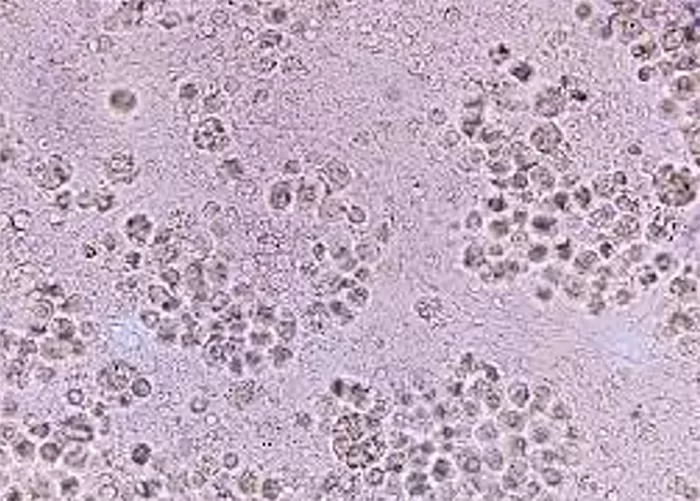
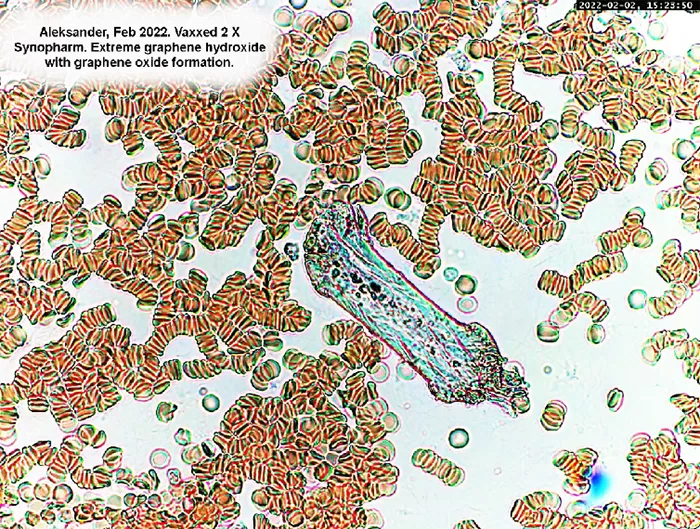
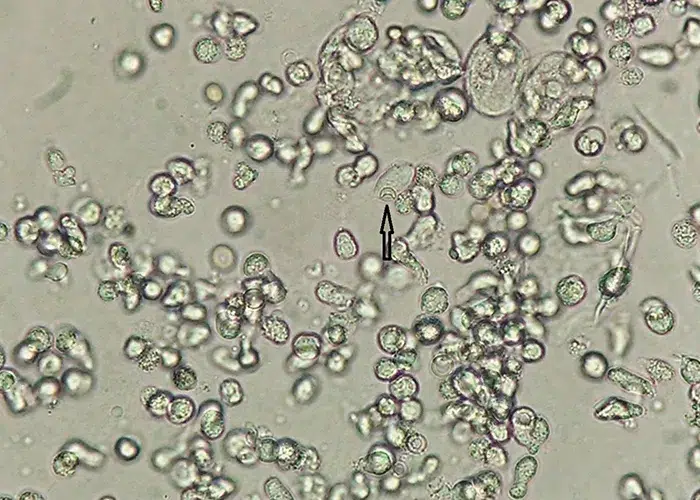
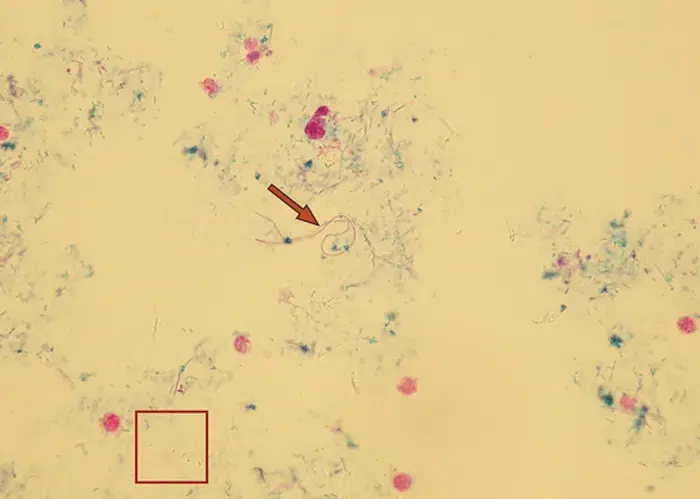
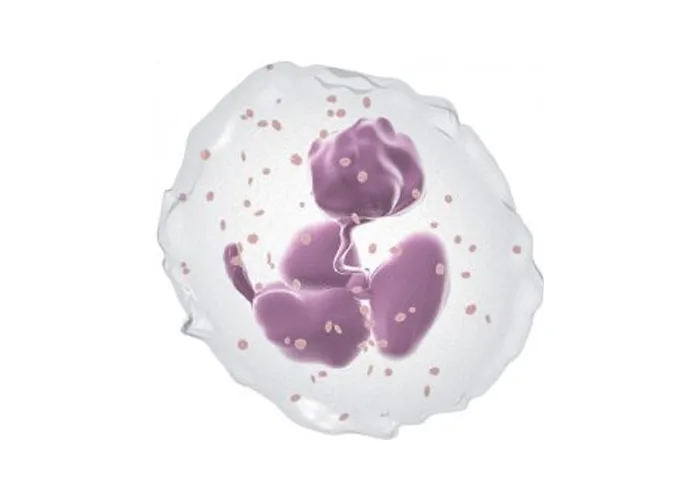
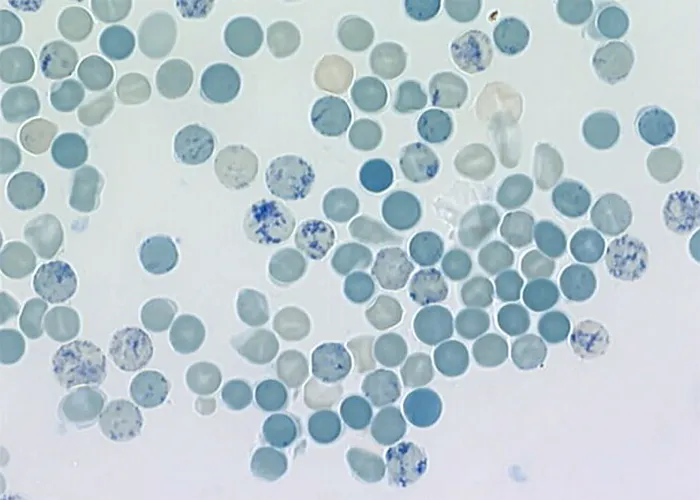
Active un-stained lymphocytes consuming pathogens, and losing cohesion while working. An indication of functioning immunities.
Some of the lymphocytes are dissolving, perhaps due to acidity of the toxin they are attempting to digest.
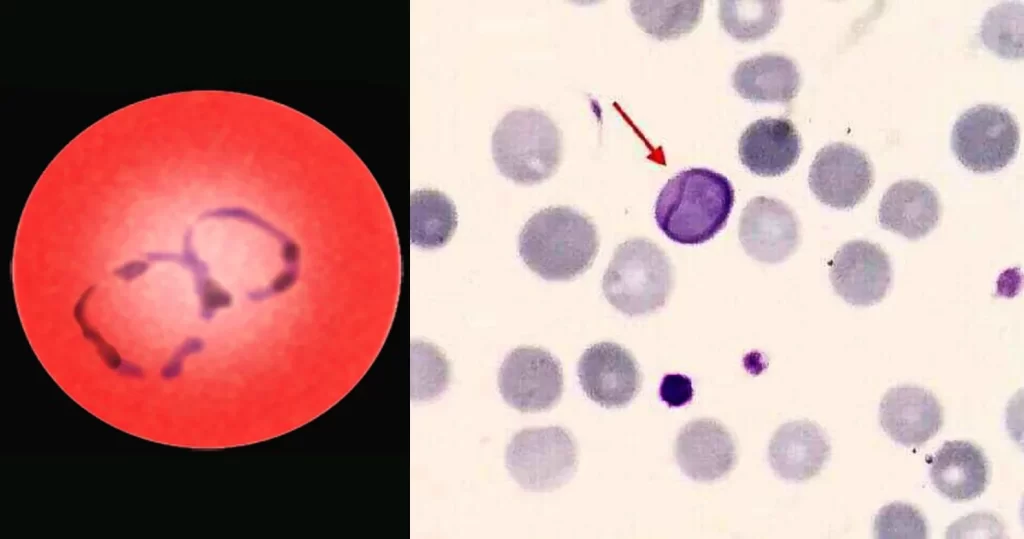
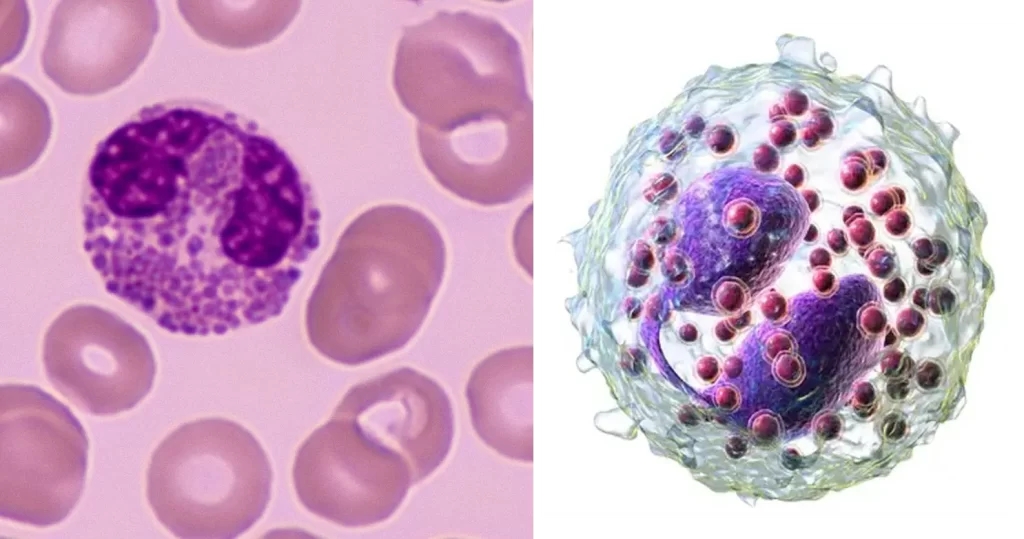
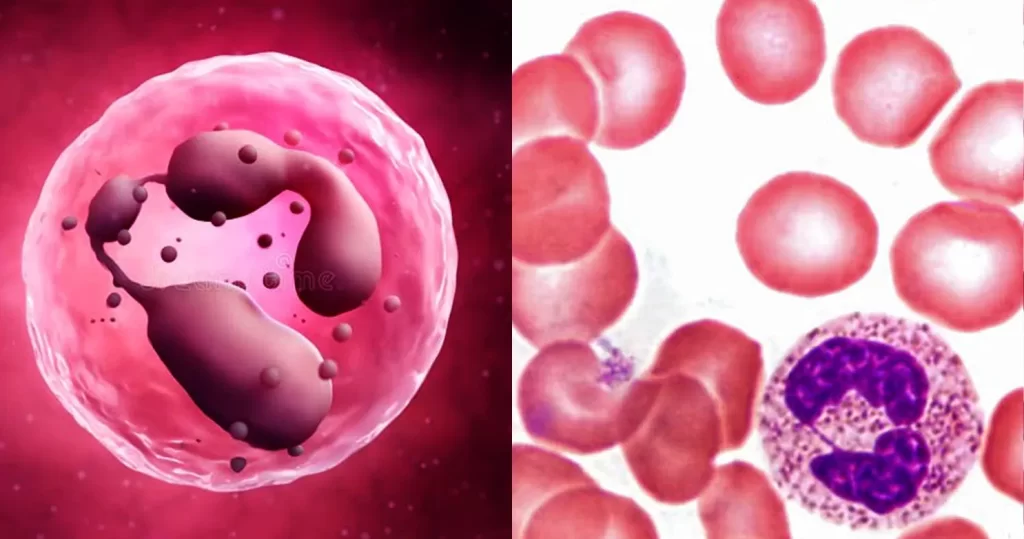
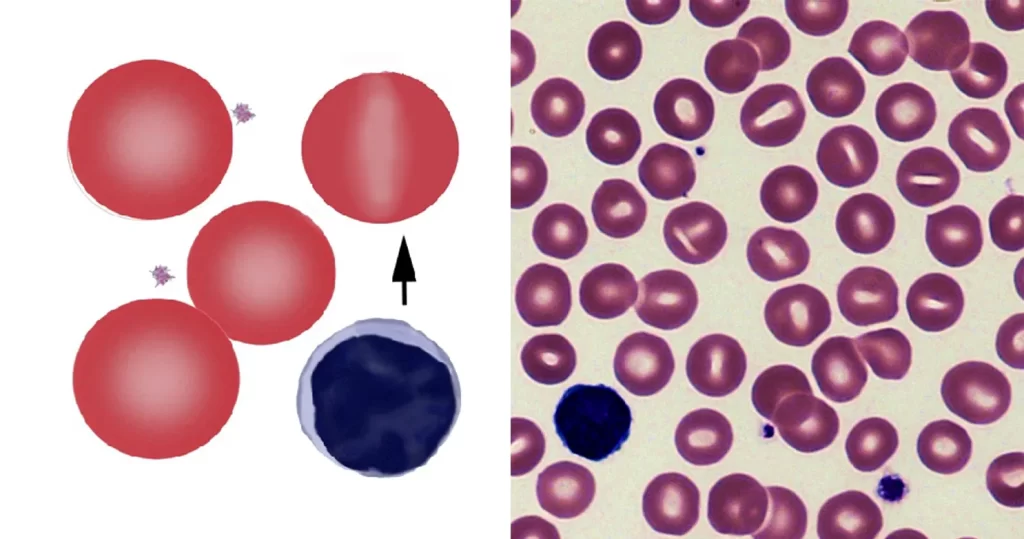
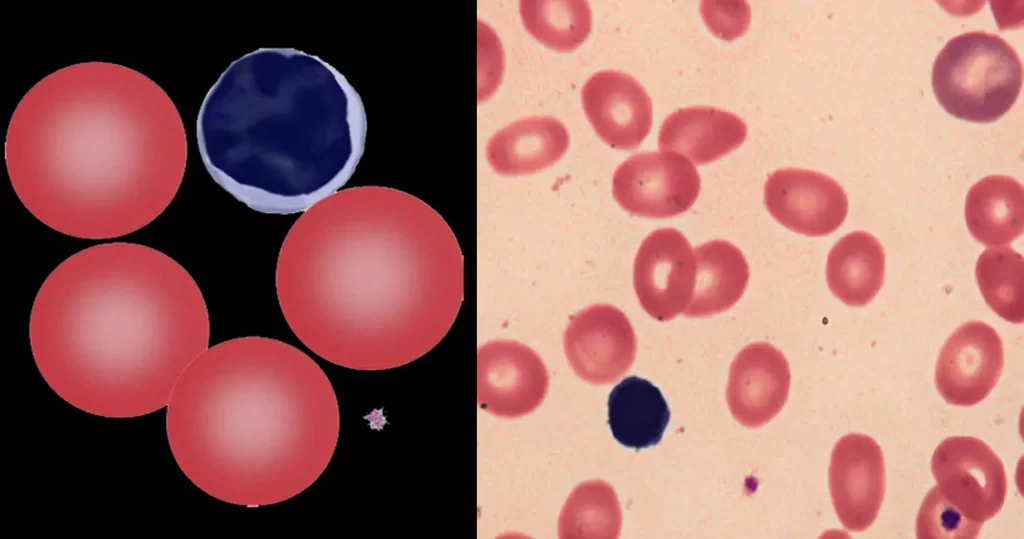
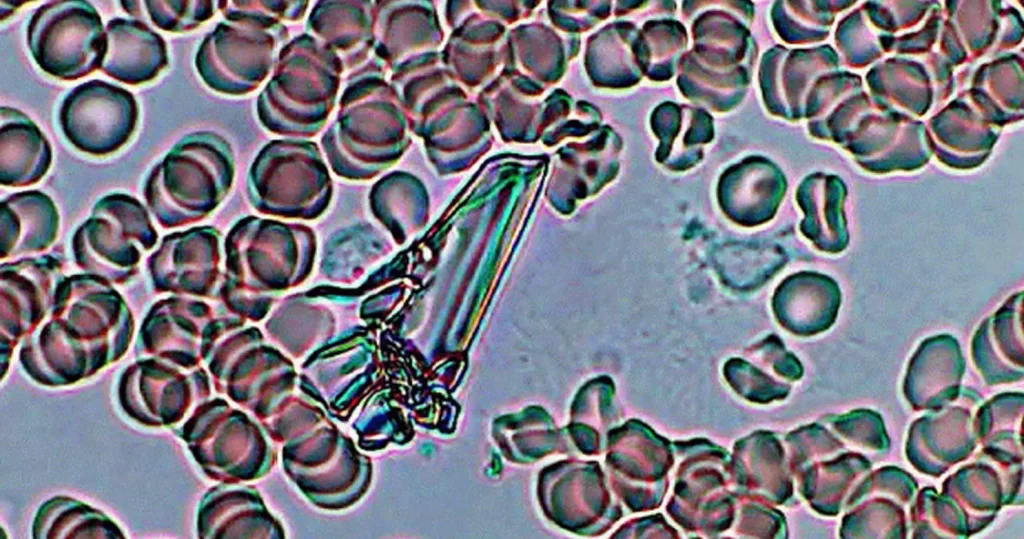
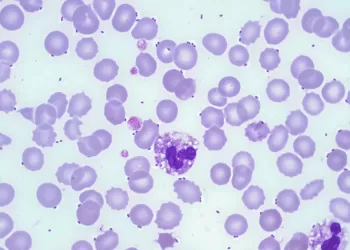
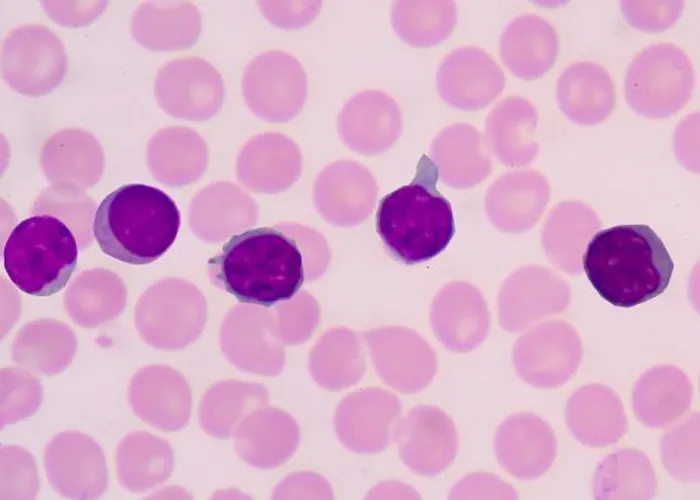
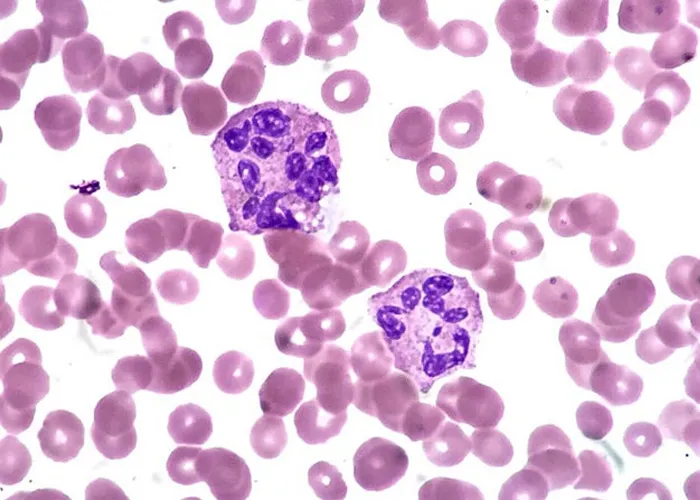
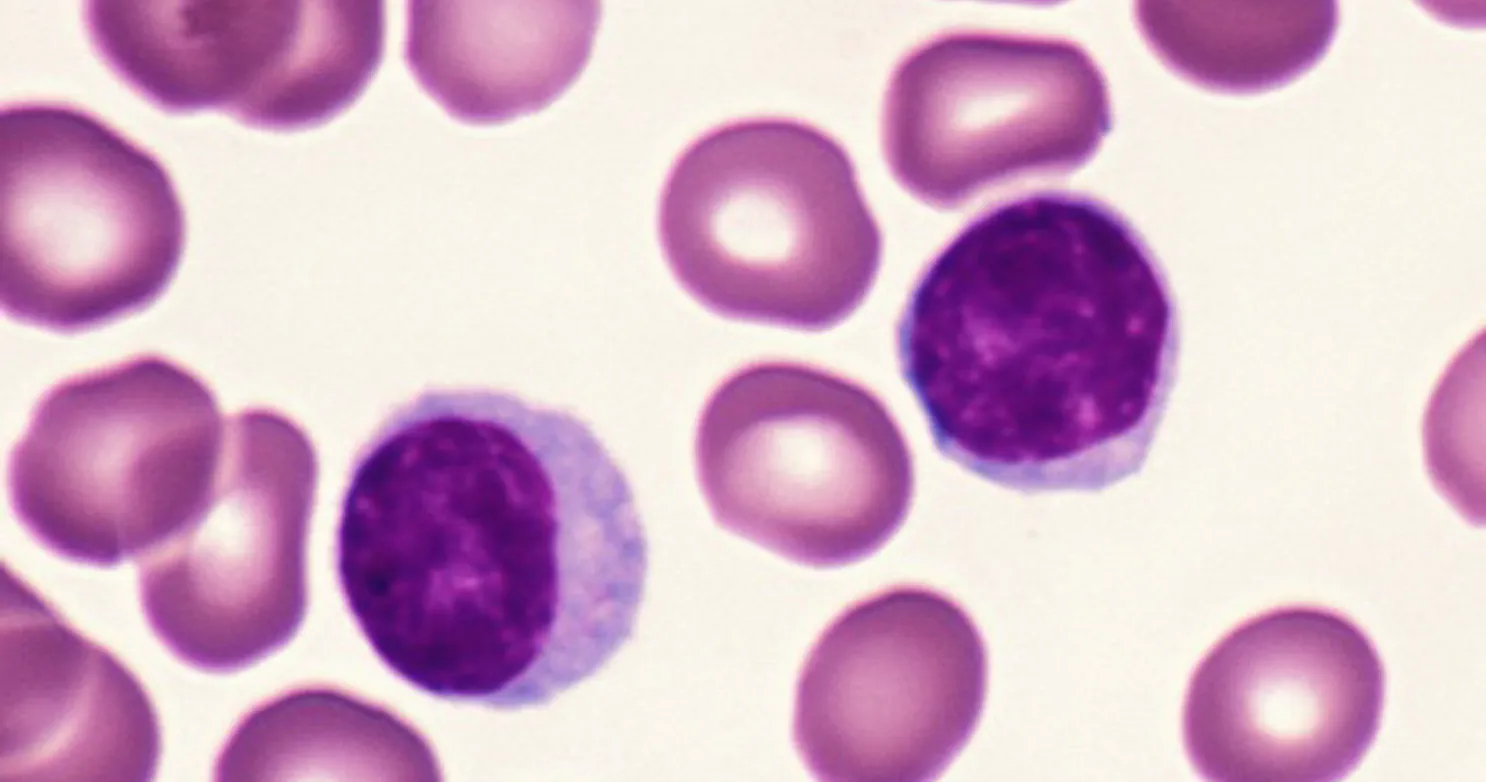
Reactive / active lymphocyte. A large cell with pale blue cytoplasm that may appear to “hug” adjacent red blood cells.
These cells are also called Downey type II cells. Indicates they are in-taking toxins from other cells, that immunities are
working. They are often increased in infectious mononucleosis due to EBV infection.
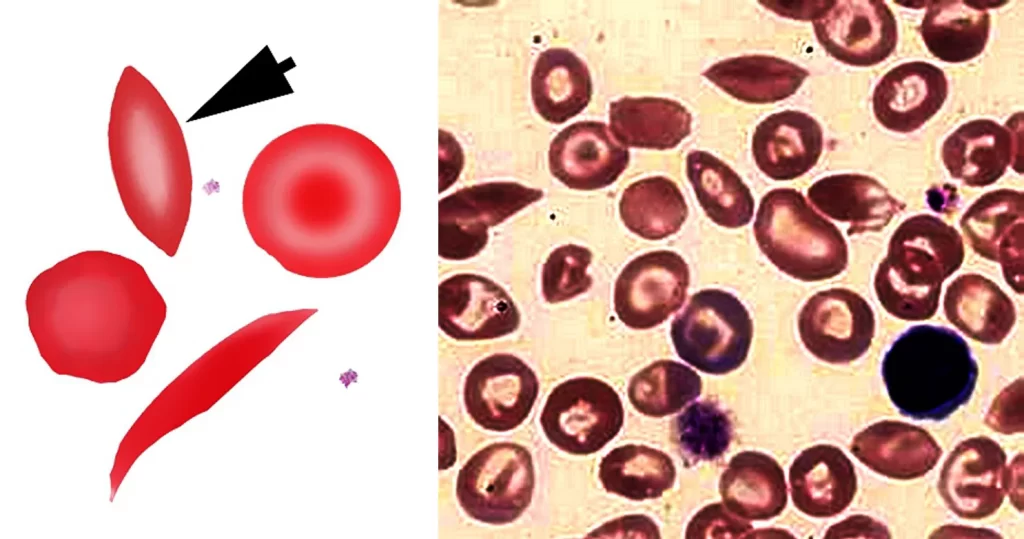
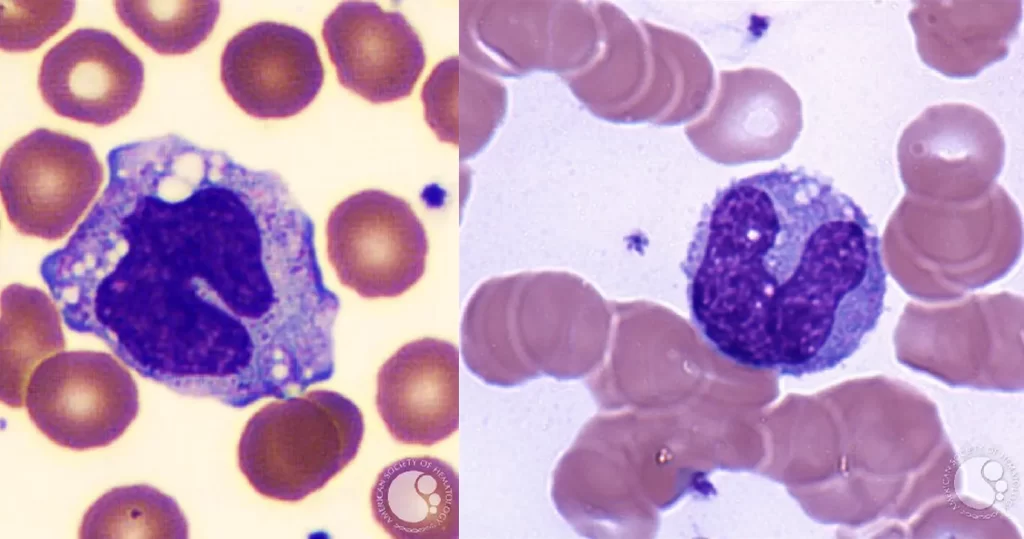
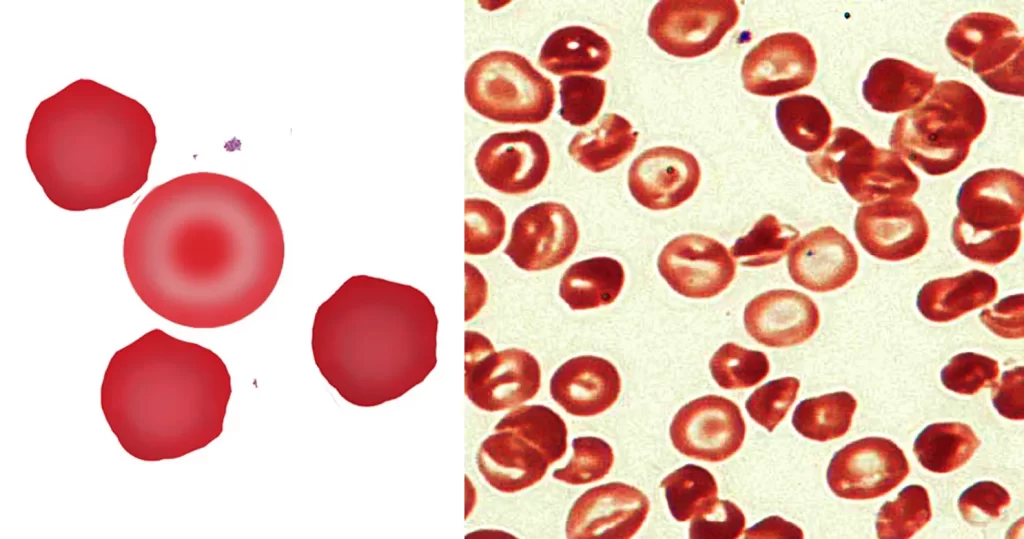
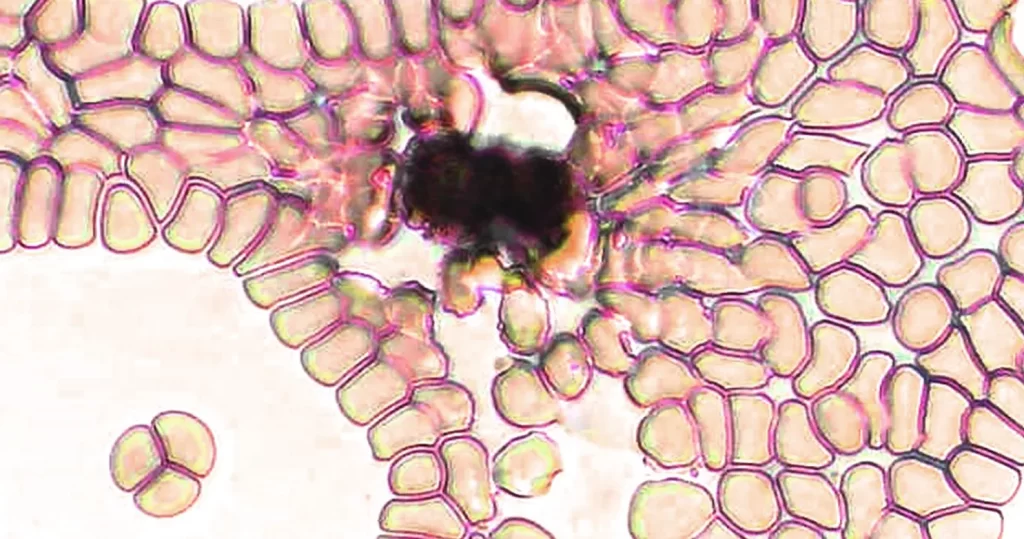
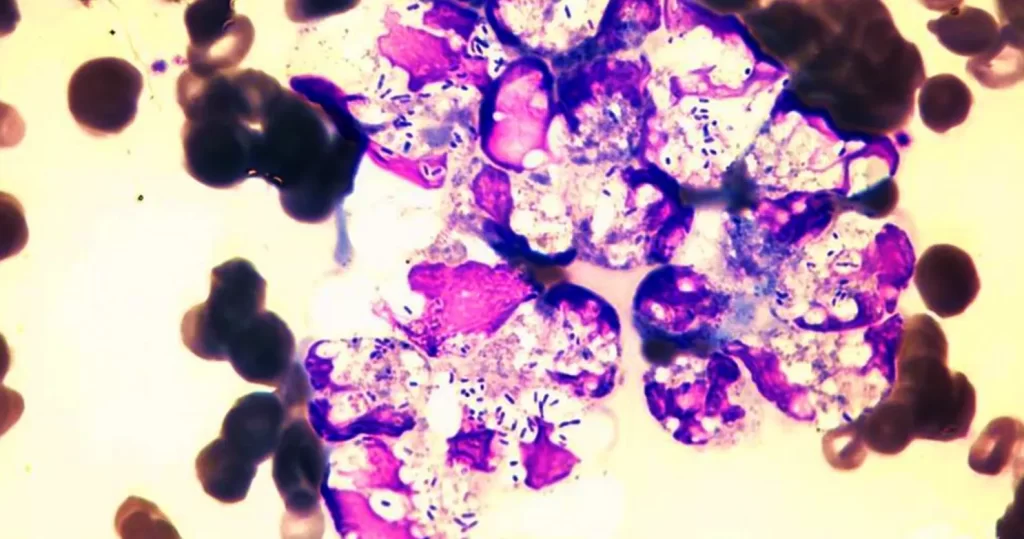
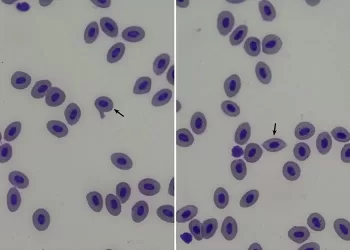
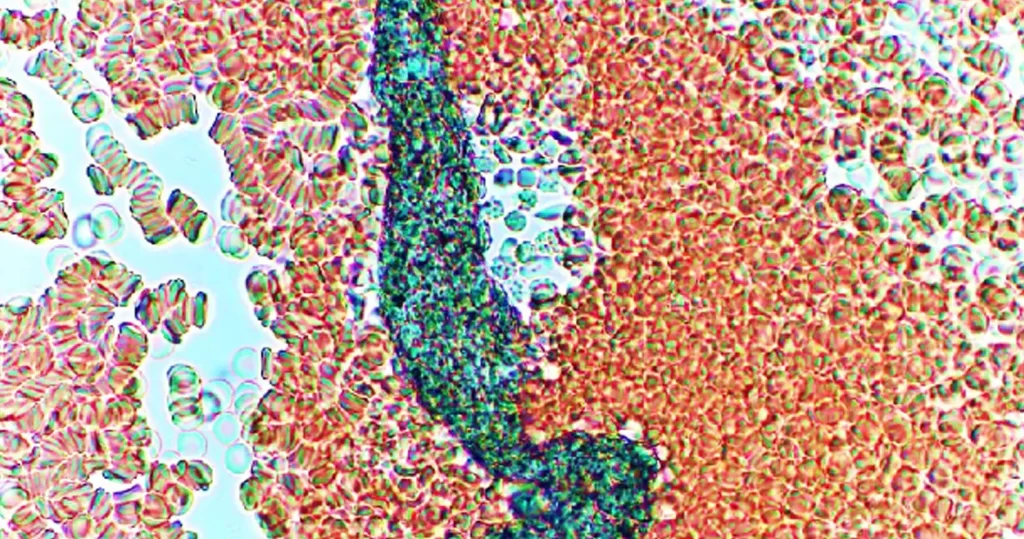
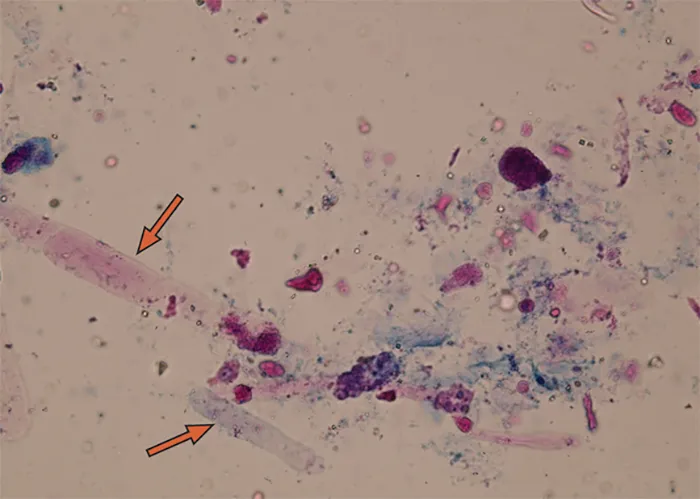
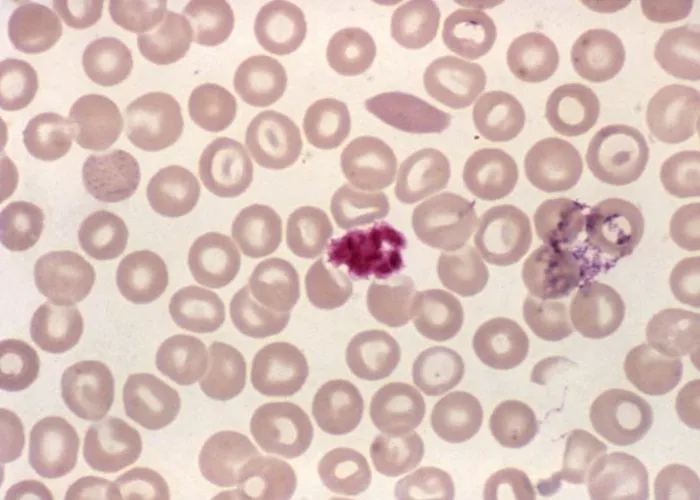
Infectious mononucleosis. The indentation of the cytoplasm of the lymphocyte (arrows) by red blood cells gives rise to the classic “Dutch skirt” appearance of the border.
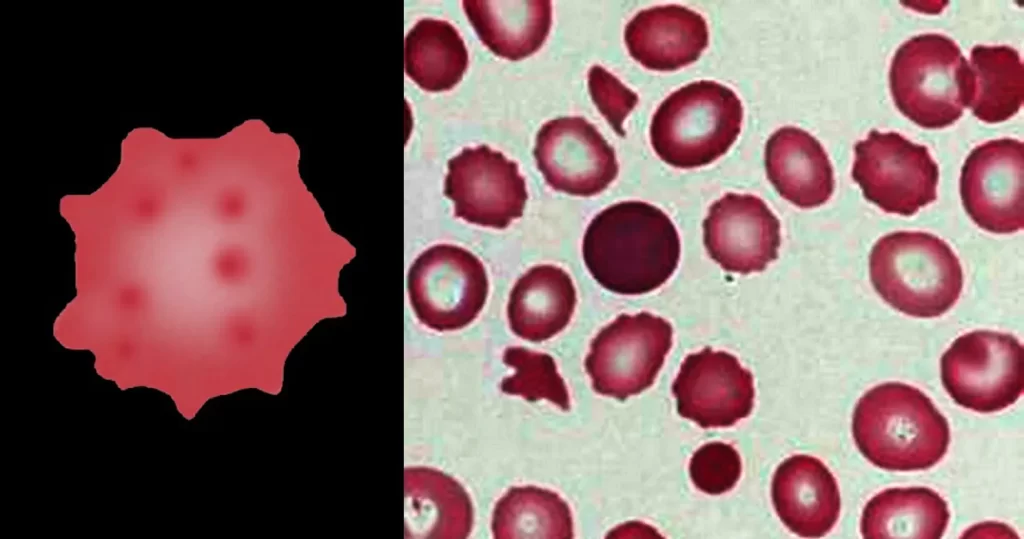
Notice how the red cells are being suctioned by the lymphocyte.
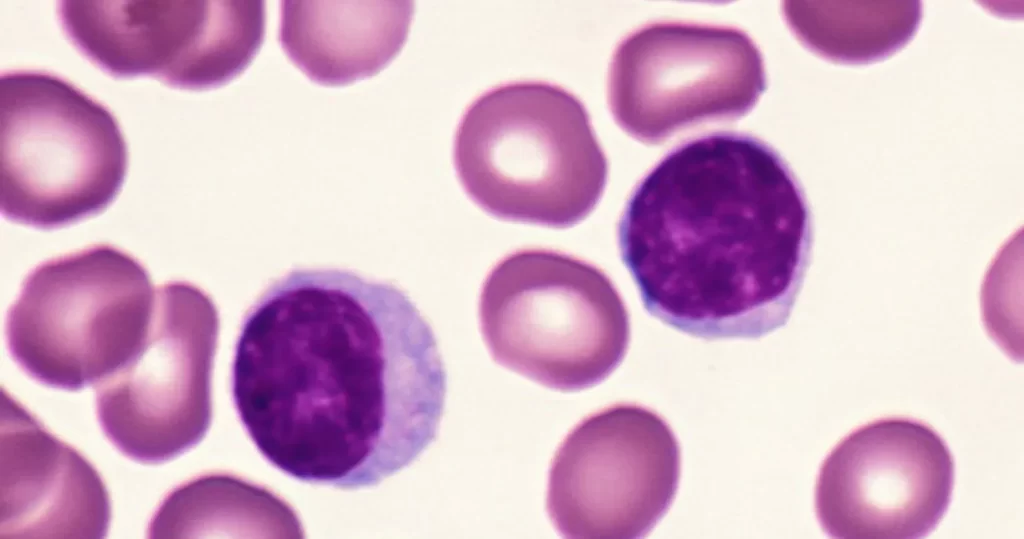
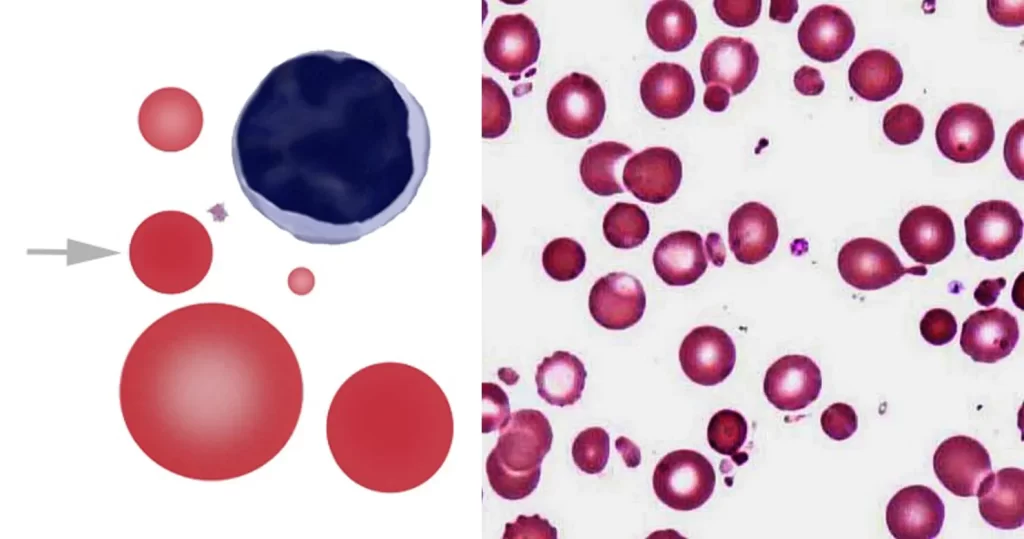
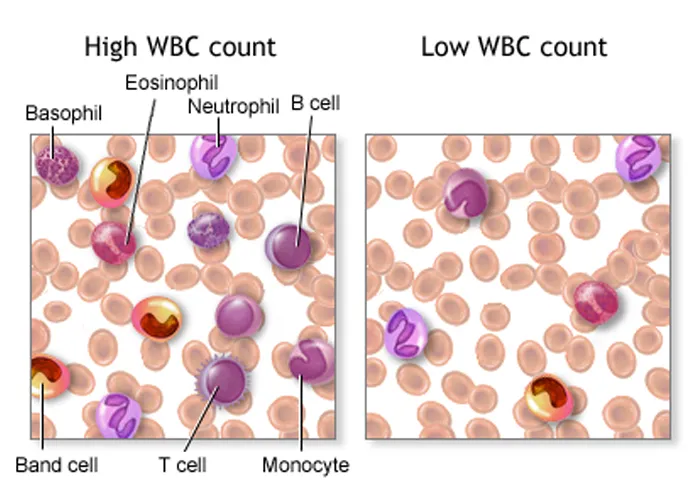
Lymphocytosis (High Levels). A feature of infection, particularly in children. In the elderly, lymphoproliferative disorders, including chronic lymphocytic leukemia and lymphomas, often present with lymphadenopathy and a lymphocytosis.
Can indicate a bacterial / fungal condition, with correspond low level of neutrophils:
- Acute viral infections, such as infectious mononucleosis, hepatitis, and cytomegalovirus
- Pertussis
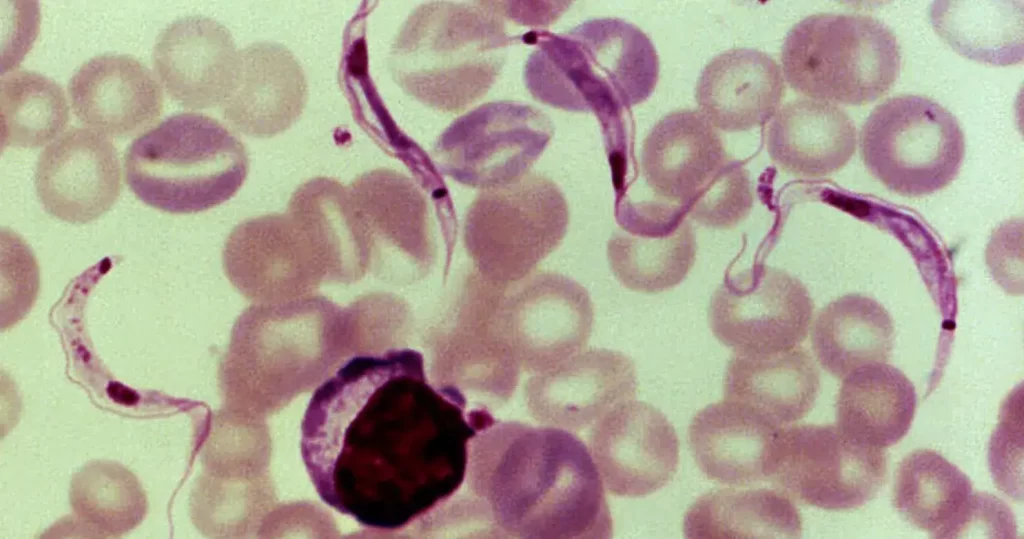
- Protozoal infections, such as toxoplasmosis and American trypanosomiasis (Chagas disease)
- Chronic intracellular bacterial infections such as tuberculosis or brucellosis
- Chronic lymphocytic leukemia
- Acute lymphoblastic leukemia
- Lymphoma
- Post-splenectomy state
- CARD11-related congenital B cell lymphocytosis (rare, also known as BENTA disease)
- Age less than 2 years
- Connective tissue diseases
- Thyrotoxicosis
- Addison’s disease
- Splenomegaly with splenic sequestration of granulocytes
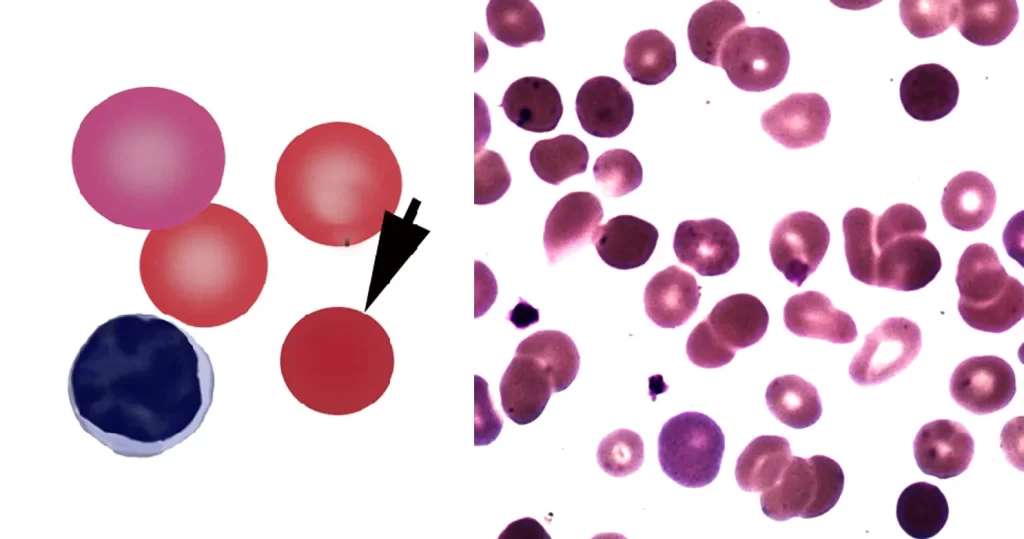
Lymphocytopenia / Lymphopenia (Low levels). The most common cause of temporary lymphocytopenia is a recent infection, such as cold or flu, otherwise known as a Herxheimer Detox Reaction.
https://en.wikipedia.org/wiki/Lymphocytopenia
Can indicate Viral conditions, often, with a corresponding increase in neutrophils
- Lymphocytopenia, but not idiopathic CD4+ lymphocytopenia
- Corticosteroid use
- HIV
- Viral, bacterial, and fungal agent,
- Malnutrition
- Systemic lupus erythematosus
- Severe stress
- Intense or prolonged physical exercise (due to cortisol release)
- Rheumatoid arthritis
- Sarcoidosis
- Multiple sclerosis
- Iatrogenic (caused by other medical treatments) conditions
- Some malignancies that have spread to involve the bone marrow
- Leukemia
- Advanced Hodgkin’s disease
- Influenza A virus subtype H1N1 (and other subtypes of the Influenza A virus)
- Monocytosis
- Large doses of ionizing radiation
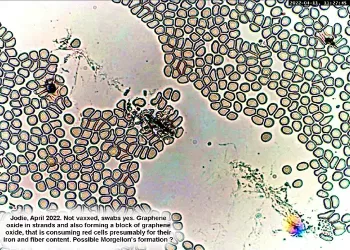
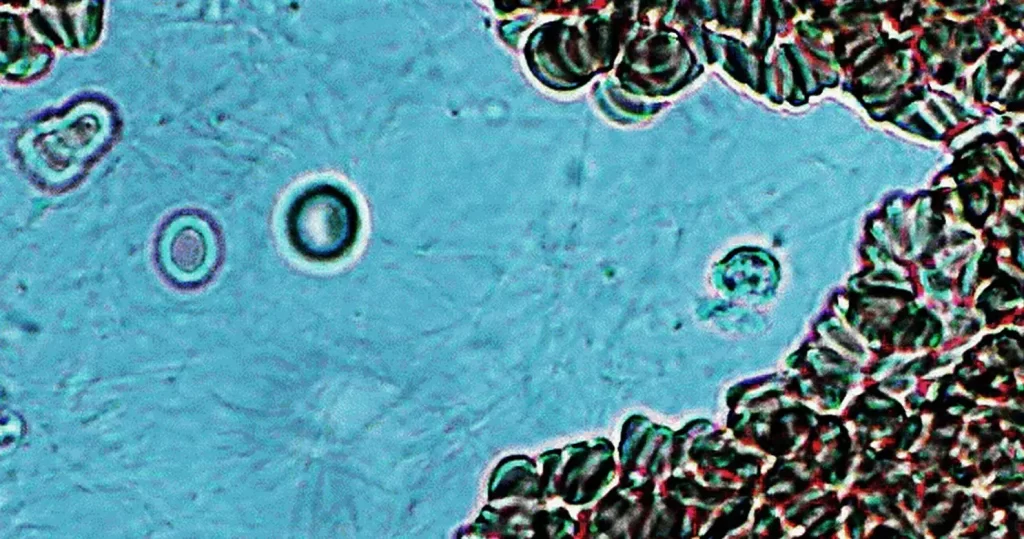
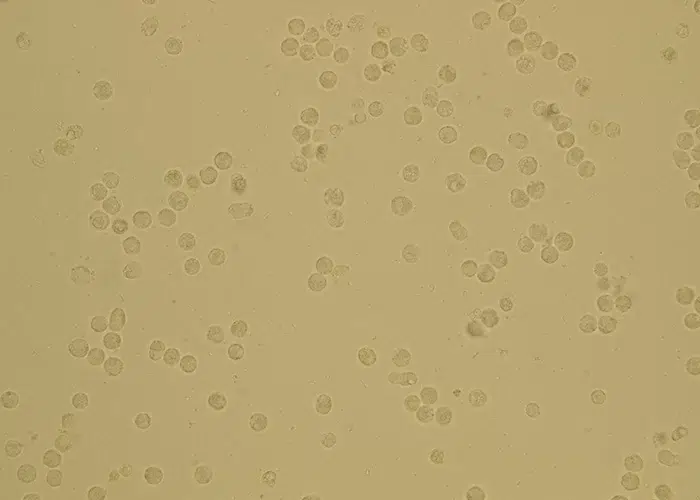
Non-active, low lymphocyte count in the scrape area of a live sample
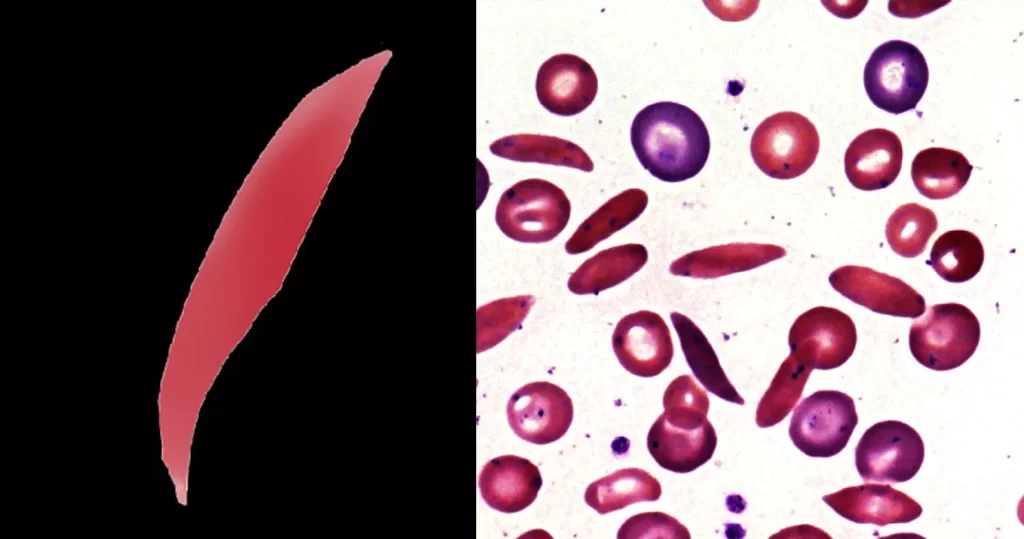
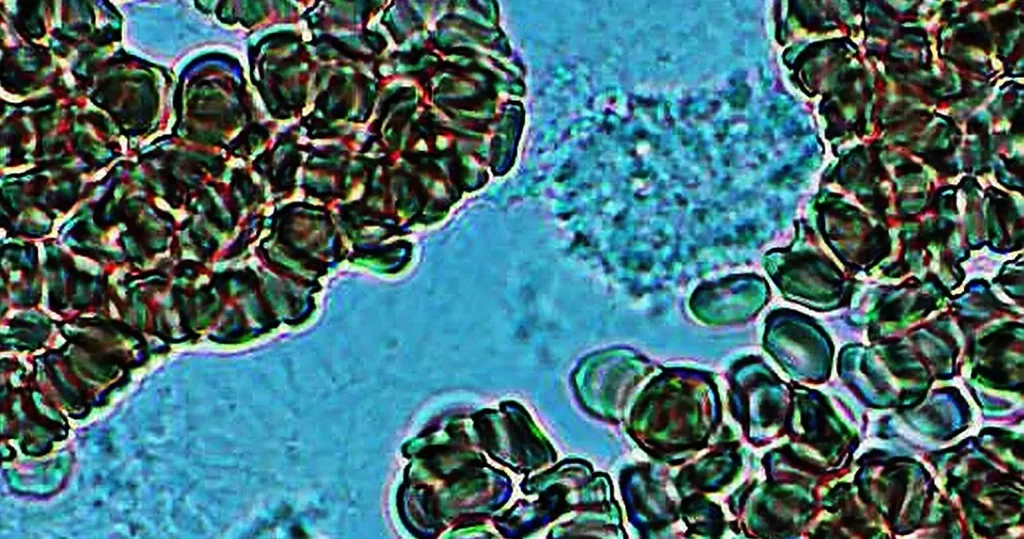
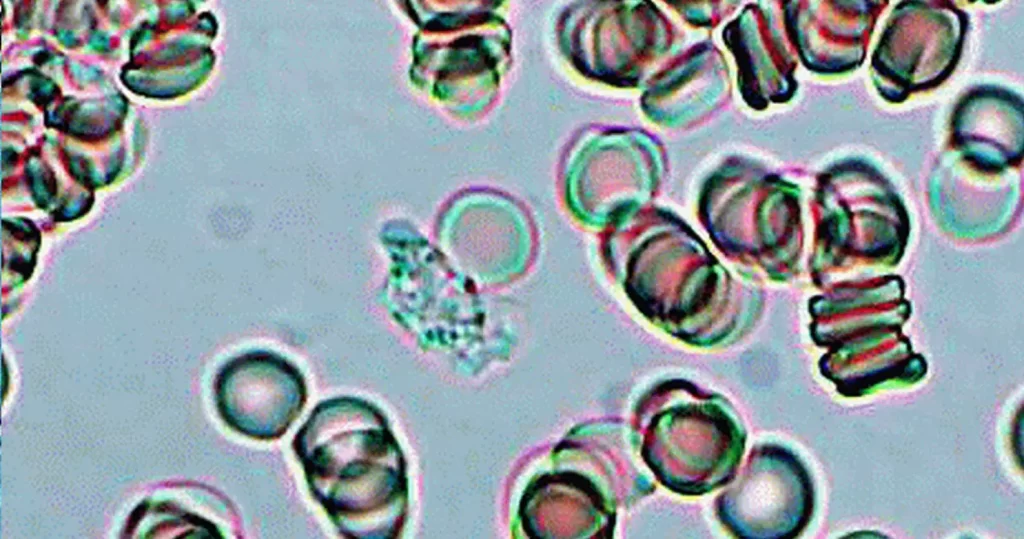
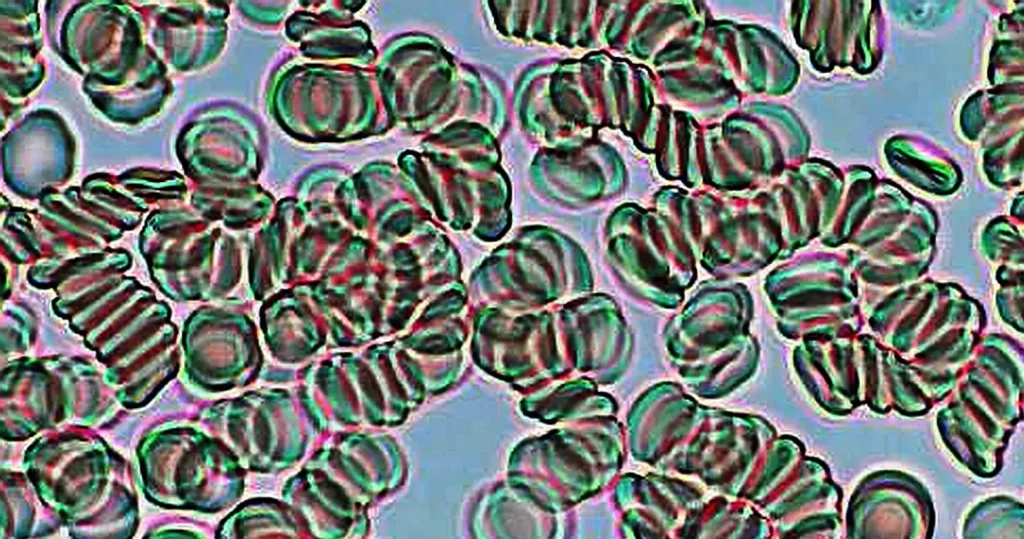
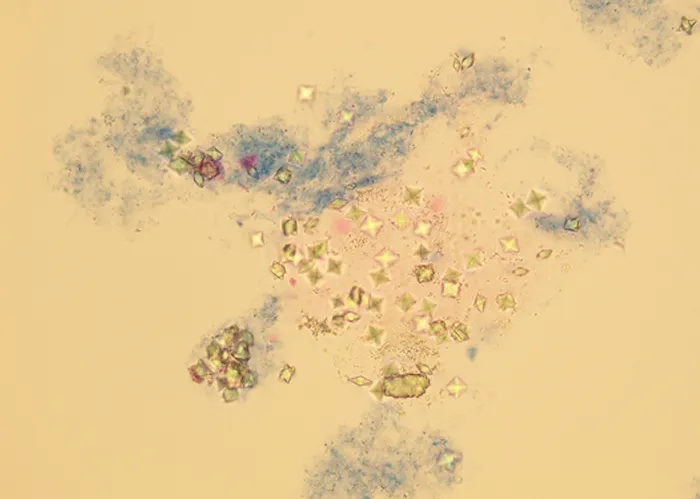
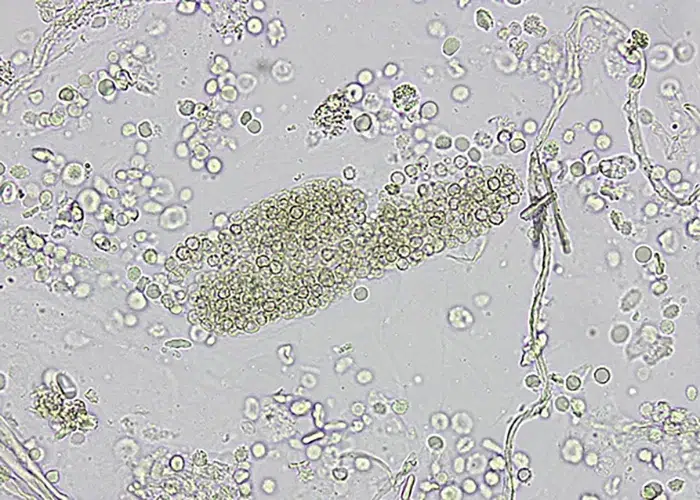
Un-stained active lymphocyte grouping, grouping around a few (larger) neutrophils.
Very toxic and darker red cells are compressed near the top and in small amounts within the sample, indicating lymphocytes are grouping to neutralize a pathogen threat.
Keep in mind that white cells do not clot, but will group when under larger threat, as though an army.